Facebook logs SMS texts and calls, users find as they delete accounts
Alex Hern,The Guardian2 hours 1 minute ago
Facebook said: ‘People are expressly asked if they want to give permission to upload their contacts from their phone.’Photograph: Kirill Kudryavtsev/AFP/Getty Images
As users continue to delete their Facebook accounts in the wake of the Cambridge Analytica scandal, a number are discovering that the social network holds far more data about them than they expected, including complete logs of incoming and outgoing calls and SMS messages.
The #deletefacebook movement took off after the revelations that Facebook had shared with a Cambridge psychologist the personal information of 50 million users, without their explicit consent, which later ended up in the hands of the election consultancy Cambridge Analytica.
Facebook makes it hard for users to delete their accounts, instead pushing them towards “deactivation”, which leaves all personal data on the company’s servers. When users ask to permanently delete their accounts, the company suggests: “You may want to download a copy of your info from Facebook.” It is this data dump that reveals the extent of Facebook’s data harvesting – surprising even for a company known to gather huge quantities of personal information.
Many other users reported unease at the data they had discovered being logged, including the contacts in their address books, their calendars, and their friends’ birthdays.
I had a similar issue with mine on Android. Don't have FB installed but I do use Messenger and Instagram. Interestingly they only tracked when I rang my parents and girlfriend. Have never used Messenger in regards to my parents. Weird.
I’ve just looked at the data files I requested from Facebook and they had every single phone number in my contacts. They had every single social event I went to, a list of all my friends (and their birthdays) and a list of every text I’ve sent.
In a statement, a Facebook spokesperson explained why contacts were uploaded. “The most important part of apps and services that help you make connections is to make it easy to find the people you want to connect with. So, the first time you sign in on your phone to a messaging or social app, it’s a widely used practice to begin by uploading your phone contacts,” it said
“Contact uploading is optional. People are expressly asked if they want to give permission to upload their contacts from their phone – it’s explained right there in the apps when you get started. People can delete previously uploaded information at any time and can find all the information available to them in their account and activity log from our Download Your Information tool.”
Facebook asks users for permission to upload this sort of personal data for a number of reasons: address books, for instance, are uploaded with the understanding that it will help users find friends on the social network and help the app’s algorithms work out how to prioritise different content. Messenger for Android asks for permissions to read call and SMS logs for a similar purpose.
The company notes that users can stop continuously uploading contacts and delete all their previously uploaded contacts by turning off the continuous uploading setting in the Messenger app.
Permanently deleting a Facebook account will also result in contacts no longer being uploaded and all previously uploaded contacts being deleted.
“Remember to look up at the stars and not down at your feet. Try to make sense of what you see and wonder about what makes the universe exist. Be curious. And however difficult life may seem, there is always something you can do and succeed at. It matters that you don’t just give up.” “In my case, medical care, personal life and scientific life are all intertwined.”
His foundation, which includes fundraising for supporting independence for those with MND - e.g. voice banking, and adapted wheelchairs.
The crisis in the health service has been created by politicians who want to privatise it – when public opinion, and the evidence, point in the opposite direction
Like many people, I have personal experience of the NHS. In my case, medical care, personal life and scientific life are all intertwined. I have received a large amount of high-quality NHS treatment and would not be here today if it were not for the service. The care I have received since being diagnosed with motor neurone disease as a student in 1962 has enabled me to live my life as I want, and to contribute to major advances in our understanding of the universe. In July I celebrated my 75th birthday with an international science conference in Cambridge. I still have a full-time job as director of research at the Centre for Theoretical Cosmology and, with two colleagues, am soon to publish another scientific paper on quantum black holes.
Last year my personal experience of the NHS and my scientific life came together when I co-signed a letter calling for healthcare policy to be based on peer-reviewed research and proper evidence. The specific issue addressed in the letter was the “weekend effect”. Jeremy Hunt, the health secretary, had claimed that thousands of patients died unnecessarilybecause of poor hospital care at the weekend, and used this to argue that we needed to implement a seven-day NHS. I had mixed feelings about the issue. Having spent a lot of time in hospital, I would like there to be more services available at weekends. Also, it seems possible that some patients spend more time in hospital than is necessary because certain diagnostic tests can only be done on weekdays.
However, as we showed in the letter, Hunt had cherry-picked research to justify his argument. For a scientist, cherry-picking evidence is unacceptable. When public figures abuse scientific argument, citing some studies but suppressing others to justify policies they want to implement for other reasons, it debases scientific culture. One consequence of this sort of behaviour is that it leads ordinary people to not trust science at a time when scientific research and progress are more important than ever.
This problem goes beyond the weekend effect. The NHS is in a crisis, and one that has been created by political decisions. These political decisions include underfunding and cuts, privatising services, the public sector pay cap, the new contract imposed on junior doctors, and removal of the student nurses’ bursary. Political decisions such as these cause reductions in care quality, longer waiting lists, anxiety for patients and staff, and dangerous staff shortages. Failures in the system of privatised social care for disabled and elderly people have placed an additional burden on the NHS.
So what is to be done? A physicist like me analyses a system in terms of levels of approximation. To a first approximation, one can see the situation facing healthcare in this country in terms of forces with different interests.
On the one hand, there is the force of the multinational corporations, driven by their profit motive. In the US, where they are dominant in the healthcare system, these corporations make enormous profits, healthcare is not universal, and it is hugely more expensive for the outcomes patients receive than in the UK. We see the balance of power in the UK is with private healthcare companies, and the direction of change is towards a US-style insurance system.
On the other hand, there is the force of the public, and of democracy. Opinion polls consistently show a majority in favour of a publicly provided NHS, and opposed to privatisation and a two-tier system. Therefore, the best way to support the NHS is to empower the public. There are two priorities. First, clear information that public provision is not only the fairest way to deliver healthcare, but also the most cost-effective. Second, a loud voice and the political power to make politicians act on our behalf.
If that all sounds political, that is because the NHS has always been political. It was set up in the face of political opposition. It is Britain’s finest public service and a cornerstone of our society, something that binds us together. People value the NHS, and are proud that we treat everyone equally when they are sick. The NHS brings out the best in us. We cannot lose it.
• Stephen Hawking, the author of A Brief History of Time, is director of research at the Centre for Theoretical Cosmology at the University of Cambridge, where he was Lucasian professor of mathematics
The danger of psychoanalysis - of no benefit, of harm, and of delaying appropriate management to aid the child and person.
Also, excellent insight into the importance of family as advocates for pushing for better care of their loved ones.
Adrien Stranieri, 20, who has autism. His mother Catherine Chavy, left, had to fight to keep him out of institutions. Photograph: Ed Alcock for the Guardian
Like thousands of French children whose parents believe they have autism, Rachel’s six-year-old son had been placed by the state in a psychiatric hospital day unit. The team there, of the school of post-Freudian psychoanalysis, did not give a clear-cut diagnosis.
Rachel, who lived in a small village outside the alpine city of Grenoble, said she would go elsewhere to assess all three of her children. But the hospital called social services, who threatened to take the children away from her.
A consultant psychiatrist said Rachel was fabricating her children’s symptoms for attention, that they were not autistic, and that she wanted them to have autism spectrum disorder in order to make herself look more interesting.
Rachel’s children were taken and placed in care homes.
The children were subsequently diagnosed with autism and other issues, proving Rachel right. But despite a high-profile court battle in which parents’ groups denounced the “prehistoric vision of autism in France”, Rachel, who herself has Asperger syndrome, has still not won back custody of her children two years later. They remain in care with limited visiting rights. Local authorities insist the decision was correct.
“I’m condemned to stand by powerless at the loss of my family,” she wrote after their latest visit to her at Christmas, fearing her children had regressed in care. “I’m destroyed, my children are destroyed.”
The “Rachel affair”, entering another courtroom appeal battle this summer, has become a symbol of what parents’ groups call the “state scandal” of the treatment of autistic children in France. The crisis is so acute that the centrist French president Emmanuel Macron has deemed it an urgent “civilisational challenge”, promising a new autism action plan to be announced within weeks.
The United Nations stated in its most recent report that autistic children in France “continue to be subjected to widespread violations of their rights”. The French state has been forced to pay hundreds of thousands of euros in damages to families for inadequate care of autistic children in recent years.
The UN found that the majority of children with autism do not have access to mainstream education and many “are still offered inefficient psychoanalytical therapies, overmedication and placement in psychiatric hospitals and institutions”. Parents who oppose the institutionalisation of their children “are intimidated and threatened and, in some cases, lose custody of their children”.
Autism associations in France complain that autistic adults are shut away in hospitals, children face a lack of diagnosis and there is a persistence with a post-Freudian psychoanalytic approach that focuses not on education but on the autistic child’s unconscious feelings towards the mother.
A 2005 law guarantees every child the right to education in a mainstream school, but the Council of Europe has condemned France for not respecting it. Pressure groups estimate that only 20% of autistic children are in school, compared with 70% in England.
“France is 50 years behind on autism,” said Sophie Janois, Rachel’s lawyer. Her book, The Autists’ Cause, published this month, sets out to raise the alarm on the abuses of autistic people’s legal rights. “Parents are told: ‘Forget your child, grieve for your child and accept the fact that they will be put in an institution’.”
“Underlying this is a cultural problem in France,” Janois says. “France is the last bastion of psychoanalysis. In neighbouring countries, methods in education and behavioural therapies are the norm and psychoanalysis was abandoned a long time ago. In France, psychoanalysis continues to be applied to autistic children and taught in universities.”
She said parents were forced to fight a constant administrative battle for their children’s rights. “There are suicides of parents of autistic children … at least five in the last couple of years.”.
The row over post-Freudian psychoanalysis and autism in France has been bitter. Eighteen months ago, a group of deputies tried and failed to make parliament ban the use of psychoanalysis in the treatment of autistic children, claiming that the “outdated” view of autism as a child’s unconscious rejection of a cold, so-called “refrigerator” mother was denying children educational support.
Psychoanalysts, who have a powerful, leading role in French mental health care, criticised the campaign as “harmful” and defamatory.
In 2012, the French health authority stated that psychoanalysis was not recommended as an exclusive treatment method for autistic people because of a lack of consensus on its effectiveness. But most state hospitals still use the methods.
In addition, the United Nations warned in 2016 that a technique called “packing” – in which an autistic child is wrapped in cold, wet sheets – amounted to “ill-treatment” but had not been legally banned and was reportedly “still practised” on some children with autism. The then health minister issued a memo advising that the practice should stop.
Parents insist that excellent professionals are present in France, but they are few and in high demand, with services patchy and varying by area.
Adrien Stranieri plays dominoes with his mother, Catherine Chavy, who privately organised support for him at home. Photograph: Ed Alcock for the Guardian
“I was told by local authorities: ‘Why are you insisting on school? Put him in an institution,’” said one mother near Tours of her high-functioning autistic seven-year-old who is now doing well academically. “In France, there is an autism of the poor, and the autism of the rich. If I didn’t have money and the skill to fight, my son would have ended up in psychiatric hospital.”
Advertisement
Catherine Chavy’s son Adrien is 20 years old. As a small child he was treated part-time at a state psychiatric hospital that used a psychoanalytical approach. His autism went undiagnosed for years. Chavy fought for a diagnosis and entry to primary school, later finding a centre that used educational and behavioural methods, where Adrien flourished. When he reached 15, there were no provisions at all. She privately organised permanent support for him at home. “He cooks, does sport, goes to his grandma’s for lunch. He has a lovely life, going out every day. If I hadn’t have done this on my own, I think he would be in an adult psychiatric hospital, tied up, on medication,” she said. “The situation in France is a health and education scandal.”
Pascale Millo set up an association for parents of autistic children in Corsica. She has a 14-year-old son, also called Adrien, with high-functioning autism and dyspraxia. The state put him in a psychiatric hospital day unit for years, but Millo didn’t get a diagnosis until he was nine. Adrien is academically strong but she has had to fight for his right, as someone with dyspraxia, to do all schoolwork on a computer, taking on the training and support herself, never sure whether, from one month to the next, lack of support in the education system will mean his studies are cut short. “In theory, France has everything: state finances, and laws to protect us,” she said. “But those laws are not being respected.”
Vincent Dennery, who heads a collective of autism associations, said he hoped for concrete, practical measures in Macron’s autism action plan, and a move from a medicalised approach towards education. “There are still thousands of autistic children in psychiatric hospital day units who have no reason to be there, but their parents can’t find any other solution,” he said.
Dennery said he felt society needed to shift. “Culturally, French society has been a place of exclusion. A large number of societies deinstitutionalised disability or difference and moved to include people in ordinary life, but France has not.”
• The bottom picture caption was amended on 14 February 2018 to correct Adrien Stranieri’s last name from Straniero.
Fifteen-minute consultation: problems in the healthy paediatrician—managing the effects of shift work on your health
FREE
Michael Farquhar
Correspondence toDr Michael Farquhar, Department of Children's Sleep Medicine, Evelina London Children's Hospital, Guy's and St Thomas’ NHS Foundation Trust, London SE1 7EH, UK; Michael.Farquhar@gstt.nhs.uk; @DrMikeFarquhar
Abstract
“You're not healthy unless your sleep is healthy”Professor William Dement, Stanford University, one of the founders of modern sleep medicine
Sleep is fundamental to good health. Healthcare professionals receive little teaching on the importance of sleep, particularly with respect to their own health when working night shifts. Knowledge of basic sleep physiology, together with simple strategies to improve core sleep and the ability to cope with working nights, can result in significant improvements both for healthcare professionals and for the patients they care for.
...
Introduction
Sleep is an essential active process.
We spend about a third of our lives asleep. We cannot survive without sleep. Getting enough good quality sleep underpins every aspect of physical and mental health. Sleep deprivation rapidly takes its toll on even the healthiest and most robust of people and can lead to an inability to function effectively.
Moderate sleep deprivation—equivalent to being awake for 16–18 hours—can have the same effect on reaction time as being at the legal blood alcohol limit for safe driving.
Up to 20% of road traffic accidents are thought to be fatigue related, and are significantly more likely to lead to serious harm or death.1
Symptoms related to poor sleep are common, particularly in healthcare professionals.
Sleep quality can be affected by other health issues, including mental health factors (eg, stress, depression), physical health factors (eg, pain) or common illnesses (eg, asthma, eczema). A primary sleep disorder (eg, obstructive sleep apnoea, restless legs syndrome, narcolepsy) may also be present. Difficulties with sleep, including problems with getting to sleep and maintaining sleep, are a common reason for adults to present to their general practitioner.
Significant sleep disruption increases risks of cardiovascular disease, diabetes and obesity, reduces the effectiveness of the immune system2 and impacts cognitive function and emotional regulation.
Despite this, most healthcare professionals receive very little education about sleep, and the importance of sleep to health.3
Thinking about healthy sleep is especially relevant for healthcare professionals, who often work shift patterns to provide essential and emergency healthcare 24 hours a day, 7 days a week, 365 days a year. Regularly working both night shifts and long daytime shifts will impact sleep routines and make achieving good quality sleep more challenging.
The ‘hero’ attitude, that patient care is always more important than appropriate self-care, is well intentioned but misguided. It is absolutely paramount that this is understood by all staff and consistently reinforced by senior clinicians and managers.
Natural sleep rhythms
We function on a natural cycle of wake and sleep. Our brains and bodies are evolved to primarily be awake by day and asleep by night.
Natural cycling of wake and sleep, circadian rhythm, is regulated by the suprachiasmatic nucleus (SCN), the primary body clock, in the hypothalamus. The SCN is affected by many cues, with the most important being environmental light. Release of melatonin, which helps regulate wake and sleep, is controlled by the SCN.
There is an independent need for sleep, which increases the longer we have been awake. This can only be reduced by sleeping, just like hunger is only reduced by eating.
When we act against our circadian rhythm we feel fatigued and function less effectively. We experience this sense of disorientation as ‘jet lag’ when we rapidly move time zones via air travel. It can take up to a day for each time zone crossed for people to regain their normal sense of wake and sleep.
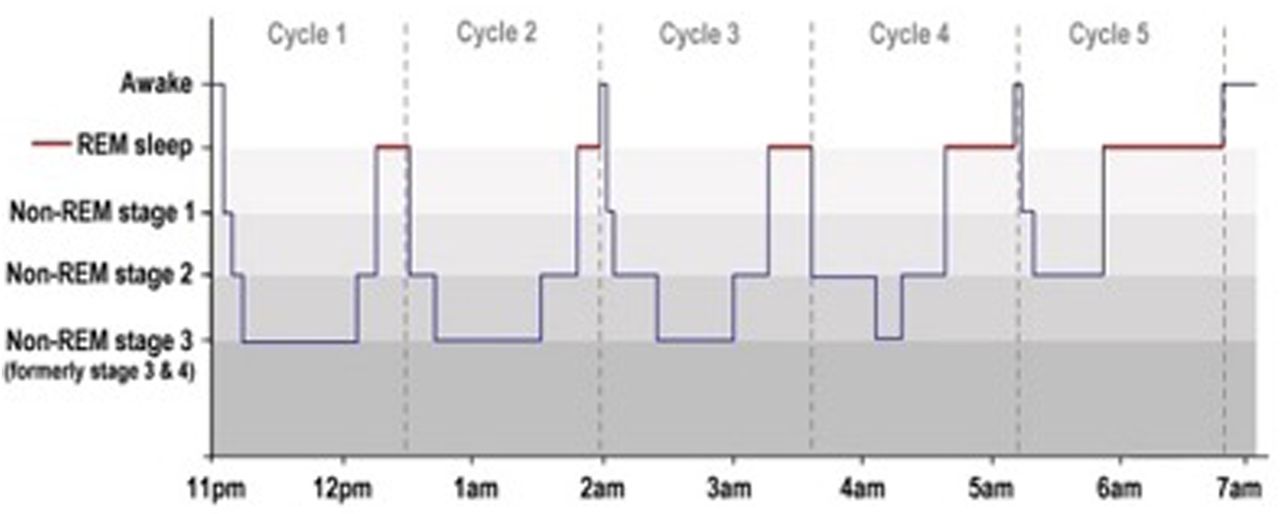
Hypnogram. REM, rapid eye movement. Adapted from Luke Mastin.
We cycle regularly through different sleep stages, principally light sleep (non-rapid eye movement (REM) stages 1 and 2), deep sleep (non-REM stage 3) and REM (or dream) sleep (figure 1).
Deep sleep is physically refreshing, and effectively ‘recharges your batteries’. REM sleep is important for consolidation of learning, and emotional regulation.
Sleep is essential for learning—getting a good night's sleep will help you retain knowledge for Membership exams far more than staying up into the early hours ever will!
Working night shifts
We are not physiologically evolved to function at night as we do in daytime, nor are we adapted to achieve good quality sleep during the day.
Working at night is equivalent to working while jet-lagged: your body is trying to function on Sydney time while your brain thinks that it is Greenwich Mean Time.
Working night shifts has associated risks and consequences (see box 1).4
Box 1
Risks and consequences of working night shifts
Night shift workers:
sleep less well and for shorter times in the day
are less alert and perform less well than day shift workers5–9
are more likely to make simple mistakes and avoidable errors, leading to increased risks to patient safety
process information, particularly novel situations, slower
have impaired alertness, vigilance and reaction time
are more likely to make decisions that involve higher degrees of risk
have increased risk of road traffic accidents after a shift10
a possible relationship with increased incidence of cancer12
The experience of feeling dangerously sleepy while driving home from work is very common among hospital night shift workers,13and continues to result in fatal outcomes for National Health Service (NHS) staff.14,15
Effects of relative sleep deprivation, fatigue and of working at night are well recognised by other professions (eg, airline pilots), and are reflected in the Highway Code.16
It is essential that professionals working night shifts, especially in intense, demanding hospital roles which require an ability to respond rapidly and to make key decisions quickly and competently, take steps to optimise their sleep and ability to function at night.
There is a personal responsibility for professionals to come to work having taken steps to ensure that they are able to function as effectively as possible.
There is also a responsibility for this to be supported by employers. Hospitals must consider strategies, particularly around night shifts, to ensure that staff are able to function at their best, and that their staff's own safety is taken into account. There is natural variation in how well individuals cope with working night shifts. Employers should consider regular screening of shift workers for health consequences of working shifts.
These ideas are not always well recognised in the NHS, which needs a significant culture shift in how to approach working at night.17
Improving sleep
Core sleep
Establishing good sleep routine and habits is the foundation of addressing sleep difficulties.
Investing time in getting sleep right every night, not just when working nights, is key to improving long-term sleep quality.
Environment
Sleep environment is important. Bedrooms should be dark, cool, quiet and comfortable.
Minimising environmental light and noise is even more important when attempting to sleep during the daytime.
Key features about good sleep environments are summarised in box 2.
Box 2
Good sleep environment
Your bed, including mattress and pillows, should be comfortable and supportive
Make your bedroom as dark as possible:
invest in blackout blinds/curtains
do not switch on main bright lights if you need to get up through the night
consider a good quality eye mask for daytime sleeping
External noise should be reduced as much as possible:
consider use of white noise (eg, a fan, quiet relaxing music, a radio turned to static)
consider use of ear plugs
your bedroom should be cool
aim for a temperature of ∼18–20°C
a warm bath, or wearing bedsocks, can encourage peripheral vasodilation before sleep, which helps to optimise core body temperature
Some natural remedies, such as lavender, can improve sleep quality
Routine and habits
Good quality sleep is maintained by regular routine.
Everyone's need for sleep is different. Most adults will need approximately 7–8 hours good quality sleep each night. If you are getting adequate sleep regularly, you should wake feeling refreshed at approximately the same time each morning whether an alarm is used or not. If you regularly ‘catch up’ sleep at the weekend or on days off, or if you often have symptoms suggestive of sleep deprivation, this implies you are not allowing enough time for sleep each night. This should be addressed as a priority.
Regularly spending time in bed awake encourages your brain to associate being in bed with wake, which can lead to difficulties in getting to sleep.
Key features about good sleep routine are summarised in box 3.
Box 3
Good sleep routine
▸ Ensure as much natural daylight exposure as possible
▸ Regular exercise, but not too close to bedtime, supports sleep—in adults with insomnia, regular exercise can be more effective than ‘sleeping tablets’ in improving sleep quality
▸ Eat regular meals
▸ Do not eat your main meal within 2 hours of bedtime
▸ A light prebed snack (eg, a bowl of cereal, fruit, yoghurt) 30 min before bed can help prevent disruption from night-time hunger, but avoid evening ‘grazing’
▸ Minimise use of alcohol, caffeine and nicotine, particularly in the evening period
▸ These can affect both the ability to get to sleep and the quality of sleep obtained
▸ Set sleep and wake times that permit the amount of sleep that is right for you
▸ Aim to go to bed at roughly the same time each night and get up at the same time each morning
Minimise electronics use for the 30–60 min before bed
▸ Consider relaxation strategies to ‘wind down’ before bed
▸ Do not use your phone as your alarm clock
▸ Your phone should preferably be charged outwith your bedroom while you sleep
▸ Avoid spending long periods of time awake in bed. Your bed should only be for sleep or sex
▸ If you are unable to sleep, get out of bed and do a quiet/relaxing activity (reading, jigsaw puzzle, building LEGO, etc) for 15 min, then return to bed and try to sleep again
Electronics
Electronic devices in the bedroom can have a major impact on sleep.18
Light, particularly at the blue end of the spectrum, has a direct effect on the primary body clock, which leads to suppression of natural melatonin secretion. Additionally, the stimulatory effect of engaging with activities when the brain is trying to wind down and relax has an inhibitory effect on sleep.
There should be an electronic curfew for at least 30–60 min before the intended bedtime. Electronic screens should be avoided in the bedroom.
If this is not possible, then enabling features, such as ‘Night Shift’ on Apple iOS devices or f.lux on other devices, which reduce the amount of emitted blue light from electronic screens in the evening, may reduce some of the impact on sleep. Brightness settings on devices should be as low as possible.
Night shifts
Improving how you function on night shifts involves thinking about preparing for the shift, the shift itself, what you do after the shift and how you recover after a run of nights (see boxes 4 and 5).
Box 4
Preparing for the night shift
▸ Maintain a good core sleep routine
▸ ‘Bank’ sleep in the 24 hours before starting nights; have a long lie, or try to have an afternoon nap
▸ Exercise in the morning may help encourage napping in the natural circadian ‘siesta time’ in the early afternoon
▸ Ensure you are well fed and well hydrated
Box 5
During the night shift
▸ Aim to stick to a consistent routine during each shift
▸ Work as a team to provide effective cover for breaks
▸ Consider use of ‘bleep filtering’ systems to minimise interruption to team members on breaks
▸ Avoid high calorie/high fat/high carbohydrate foods—night shift calories DO count, and contribute significantly to increased risks of impaired glucose tolerance and cardiovascular disease of working night shifts
▸ Try to maintain your normal eating patterns/times as much as possible when working nights
▸ Aim to minimise eating between 24:00 and 06:00 where possible, and when you do eat/snack choose healthier satisfying options (eg, soups/ wholegrain sandwiches/yoghurt/fruit/salads/nuts, etc)
▸ Keep well hydrated; carry a water bottle and drink regularly
Maximise exposure to bright light in non-clinical areas
▸ Your patients need their sleep—keep light and noise disruption in clinical areas to a minimum
Your breaks are essential
▸ During breaks, have short (15–20 min) naps
▸ Use caffeine carefully
▸ Watch the 4 am dip. This is when both you and your patients are at their lowest physiological ebb. Take time to double check all critical calculations in particular
Rest, breaks and naps
Breaks are not a luxury, especially when doing busy or intense night work.
Regular rest is essential to ensure safe, effective patient care is delivered to the best of your capability. Unless critically ill patients require immediate attention, your patients are always better served by clinicians who have had appropriate periods of rest during their shift.
Use breaks to take short naps; 15–20 min naps during night shift can have significant positive benefits. They can significantly improve levels of alertness and responsiveness19 and can reduce the risks to your health of working night shifts. They help to reduce risks to patients as a result of fatigued professionals.
The right length of short nap will vary between individuals. It is worth doing some experimentation to find the best for you. Longer naps are not better, as they may result in you entering deeper stages of sleep which can be more difficult to quickly wake from and increase the chance of ‘sleep inertia’ (grogginess on waking). Set an alarm, or ask a colleague to wake you.
Prolonged sleep during a single night may also affect your ability to sleep during the day, which is particularly relevant when doing consecutive night shifts.
Not everyone is able to ‘power nap’ in this fashion, in which case relaxation in a dark, quiet room may also be of some benefit.
Naps during night shift breaks are supported by the Royal College of Physicians, the Royal College of Nursing and the British Medical Association.20–22
Caffeine
Use caffeine carefully. Caffeine increases alertness23 but too much can lead to irritability and reduced effectiveness. Caffeine can reduce subsequent sleep quality and duration up to 6 hours after ingestion, so aim to use it mainly in the earlier part of your night shift.
Taking caffeine just before a planned short nap maximises its impact; caffeine takes 15–20 min to take effect, meaning it is just kicking in as you wake up at the end of your nap to give you a double boost.
▸ If possible wear sunglasses on the way home—daylight will encourage your brain to feel awake and reduce your chance of getting good quality sleep
Be cautious of wearing sunglasses if driving however
▸ Aim to be in bed as quickly as possible after your shift ends—the later you get to sleep, the less total sleep you are likely to get
▸ Resist the temptation to use electronic devices
▸ Have a light meal/snack about 30 min before going to sleep—do not go to bed hungry
▸ Avoid alcohol, nicotine and caffeine
▸ If you share a house/flat with other people, make sure they clearly know you are trying to sleep
▸ Do not allow daytime deliveries during the time you expect to be asleep
▸ Your phone should preferably be in a different room in airplane mode
▸ On waking ensure you are exposed to bright light for the first 20 min after waking
▸ Try to do some light exercise
Once awake for ∼16–18 hours, reaction times are likely to be similar as if you are at the legal drink-drive limit. Your ability to safely drive, and your judgement as to whether you think you can are impaired.
Employers should have a policy on how to assist staff who feel too tired to safely drive. If alternative provisions (eg, public transport) are not possible, then ideally a bed should be provided, free of charge, for you to have enough sleep to then be able to safely drive home. You should be aware of your employer's policy.
Recovery
You will have slept less, and less well, while you are on nights.
Your priority should be to re-establish your normal routine as quickly as possible.
▸ Postnights team breakfasts are not just a social event. They allow you to informally ‘decompress’ and reflect on events which may have occurred during your shifts. Airing worries and anxieties in a supportive environment will likely help you sleep better
▸ After your final night, aim for a short morning nap (1–2 hours), ideally before midday, then get up and do as many ‘normal’ activities as possible
Re-establish normal eating and exercise patterns
▸ Aim for as close to your normal bedtime as possible
▸ Aim for a short lie in only on the following morning; try to get up as close to your normal wake time as possible, and to go to bed only slightly earlier than usual
▸ You are likely to need two ‘normal’ nights to successfully re-establish your usual sleep pattern
▸ …remember your judgement is likely to be a bit impaired after nights, so beware the attraction of the postnights spending spree!
How can hospitals make things better?
While professionals have a personal responsibility to ensure they are able to function during night shift to work as effectively as possible, employers also have a responsibility to support their staff. Simple interventions can make big differences.
Where health services are under increasing pressure, even basic measures to support staff can be difficult to achieve. Nevertheless, attention to appropriate, adequate rest and other factors to improve performance during night shifts are not areas where compromise can safely be made. The attendant risk of fatigue-related error rapidly escalates when working in pressured medical environments.
It is absolutely paramount this is acknowledged and actively supported by senior healthcare and clinical leaders. See box 8.
Box 8
How can hospitals make things better?
▸ Use forward-rotating (day-evening-night) rota designs
▸ Minimise frequent transitions between day and night shifts
▸ Provide adequate recovery time after nights to re-establish normal wake/sleep patterns
▸ Provide basic education for staff at induction regarding sleep and working nights, as well as general healthy lifestyle advice and support
▸ Ensure staff are compliant with current rest/break entitlement requirements:
Current ‘New Deal’ contract: at least 30 min continuous rest after approximately 4 hours duty
New contract: at least one 30 min paid break for a shift rostered to last more than 5 hours and a second 30 min paid break for a shift rostered to last more than 9 hours
▸ Encourage team-based ‘hospital at night’ approach, including bleep filtering and protection policies to permit consistent breaks
▸ Provide appropriate rest areas (not necessarily an ‘on-call room’) overnight, which allow staff to nap during breaks if they choose to
▸ Provide access to good quality food for night staff
▸ Provide beds, free of charge, for postnights staff who feel too tired to drive home
▸ Offer regular screening of shift workers for primary sleep disorders
Get help if you need it
Doctors and other healthcare professionals are at increased risk of having formal sleep disorders. If you think you have a genuine sleep problem, see your own doctor or occupational health service. Do not ignore it—it will often just get worse.
Avoid the temptation to self-medicate, whether with prescription medication or non-prescription options, such as alcohol, sedative antihistamines or non-prescribed melatonin.
Conclusion
Finding a pattern of wake and sleep in preparation for, while working, and recovering from night shift is a very individual process. There are no universal ‘magic bullets’ that will improve the experience for everyone.
Simple strategies by both professionals and employers to support core sleep and while working night shifts are likely to make working nights a bit less challenging and to improve both personal health and patient safety.
Further reading: A more comprehensive list of references is included in the Royal College of Physicians summary document ‘Working the Night Shift’.17
. Effect of reducing interns’ work hours on serious medical errors among interns in intensive care units. N Engl J Med 2004;351:1838–48. doi:10.1056/NEJMoa041406
. Effect of sleep deprivation on the performance of simulated laparoscopic surgical skill. Am J Surg 2003;186:169–74. doi:10.1016/S0002-9610(03)00183-1
. Night-shift work and risk of breast cancer: a systematic review and meta-analysis. Breast Cancer Res Treat 2013;138:291. doi:10.1007/s10549-013-2433-1
. Effects of napping on sleepiness and sleep-related performance deficits in night-shift workers: a systematic review. Biol Res Nurs 2014;16:134–42. doi:10.1177/1099800413476571




{kind=link}